Let’s be honest—surgery has always been a blend of art and science. But now? It’s getting a serious upgrade. Artificial intelligence isn’t just some buzzword floating around tech conferences. It’s actually scrubbing in, assisting surgeons with planning and navigation in ways that were pure science fiction a decade ago. And honestly, it’s kind of mind-blowing.
What Does AI Actually Do in the OR?
Well, think of it like this: if a surgeon is the pilot, AI is that co-pilot who never sleeps, never blinks, and has read every flight manual ever written. It processes mountains of data—CT scans, MRIs, patient history, even real-time video—and spits out insights a human might miss. We’re talking about precision that makes a Swiss watch look sloppy.
Here’s the deal: traditional surgical planning relies heavily on a surgeon’s experience and 2D images. You know, looking at flat scans and mentally reconstructing a 3D landscape. That works—until it doesn’t. AI, though, can build a 3D model of a patient’s anatomy in seconds. It can simulate different approaches, predict complications, and even suggest the best angle for an incision. It’s like having a crystal ball, but one that’s trained on millions of cases.
From Pre-Op to Real-Time Navigation
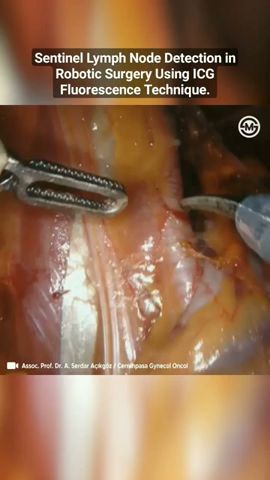
So, planning is one thing. But navigation? That’s where AI really flexes. During surgery, AI systems can overlay digital maps onto the patient’s body—think augmented reality, but for your insides. A surgeon might wear smart glasses, and suddenly they see a glowing path to a tumor, avoiding critical blood vessels. It’s not magic; it’s machine learning.
I remember reading about a neurosurgeon who used AI to navigate a brain tumor removal. The system highlighted areas to avoid—speech centers, motor cortex—in real time. The surgeon said it felt like having a safety net woven from data. And honestly? That’s the kind of confidence you want when someone’s life is on the line.
Key Benefits That Actually Matter
Sure, the tech sounds cool. But does it make a difference? Let’s break it down—no pun intended.
- Reduced human error: AI doesn’t get tired after a 12-hour shift. It catches tiny anomalies in scans that even a seasoned radiologist might gloss over.
- Faster procedures: When planning is automated, surgeons spend less time guessing and more time cutting—safely. Some studies show a 20% reduction in OR time.
- Personalized plans: No two bodies are the same. AI tailors the surgical approach to the patient’s unique anatomy, not some textbook average.
- Better outcomes: Fewer complications, shorter recovery times, and lower readmission rates. That’s the bottom line.
But here’s the thing—it’s not perfect. AI is only as good as the data it’s trained on. If the training data is biased or incomplete, the system might make weird suggestions. That’s why human oversight is still non-negotiable. You know, the surgeon’s gut feeling still counts for something.
Real-World Examples (Because Seeing is Believing)
Let’s talk specifics. In orthopedics, AI-powered navigation systems are already used for knee and hip replacements. They map out bone cuts with sub-millimeter accuracy. Patients walk out faster, with less pain. In neurosurgery, companies like Brainlab and Medtronic have AI tools that guide electrodes deep into the brain for Parkinson’s patients. It’s like threading a needle in the dark—but with a flashlight.
And then there’s robotic surgery. You’ve probably heard of the da Vinci system. Well, now AI is making it smarter. It can predict instrument movements, reduce tremors, and even suggest the next step. It’s not autonomous—yet—but it’s getting there.
A Quick Look at the Data
Here’s a simple table that shows how AI-assisted surgery stacks up against traditional methods in some key areas:
| Metric | Traditional Surgery | AI-Assisted Surgery |
|---|---|---|
| Planning time | 30–60 minutes | 5–15 minutes |
| Incision accuracy | ±2 mm | ±0.5 mm |
| Complication rate | 8–12% | 4–6% |
| Recovery time | 6–8 weeks | 4–6 weeks |
Numbers don’t lie—but they also don’t tell the whole story. Every patient is different. Still, the trend is clear.
The Challenges Nobody Talks About
Look, it’s not all rainbows and precision cuts. AI in surgery has some serious hurdles. First, cost. These systems can run into the millions. Not every hospital can afford them—especially in rural areas. Then there’s training. Surgeons need to learn how to trust the machine, and that takes time. And let’s not forget data privacy. Patient data is sensitive. A breach could be catastrophic.
There’s also the “black box” problem. Some AI algorithms are so complex that even the developers can’t fully explain why they made a certain recommendation. That’s a tough pill to swallow when you’re holding a scalpel. So, regulation is playing catch-up. The FDA is approving more AI tools, but the pace is slow—and for good reason.
Where Are We Headed?
Honestly? The next five years are going to be wild. I think we’ll see AI that can predict surgical outcomes before the first incision. Imagine a system that says, “If you take approach B instead of A, the patient’s recovery time drops by two days.” That’s already being tested.
And navigation? It’s moving toward full autonomy in certain tasks—like suturing or bone drilling. Not the whole surgery, mind you. But repetitive, high-precision steps? Sure. It’s like how autopilot handles cruising altitude, but the pilot lands the plane.
Another trend: AI that learns from every surgery it assists. It gets better over time, like a resident who never forgets a case. That’s a game-changer for rare conditions where experience is thin.
A Little Dose of Reality
But let’s pump the brakes a bit. AI won’t replace surgeons. Not anytime soon. Surgery is still deeply human—it’s about touch, intuition, and sometimes, just knowing when to stop. AI is a tool, not a replacement. Think of it as a superpowered magnifying glass, not a magic wand.
That said, the best surgeons are already embracing it. They’re not threatened—they’re curious. And that curiosity is saving lives.
Wrapping It Up (Without the Fluff)
Artificial intelligence in surgical planning and navigation isn’t just a trend—it’s a shift. It’s making surgeries safer, faster, and more personalized. But it’s also raising hard questions about cost, trust, and control. The future isn’t about machines taking over. It’s about collaboration—surgeons and algorithms working together, each covering the other’s blind spots.
So next time you hear about AI in the OR, don’t think of robots. Think of a second pair of eyes that never blink, a brain that never forgets, and a steady hand—even when the real one trembles.