Imagine a surgeon trying to find a single, tiny, glowing needle in a haystack. That’s kind of what sentinel lymph node mapping used to feel like. Except the needle is a lymph node, and the haystack is… well, a patient’s body. But now? We’ve got a flashlight. Actually, we’ve got something way better — intraoperative fluorescence imaging. It’s changing the game, honestly. Let’s dive into how this tech works, why it matters, and where it’s headed.
What Exactly Is Sentinel Lymph Node Mapping?
Here’s the deal: when cancer spreads, it often travels first to a specific lymph node — the sentinel node. Think of it as the “guardian” of the lymphatic system. If that node is cancer-free, there’s a good chance the cancer hasn’t spread further. So, finding it is critical for staging and treatment decisions.
Traditionally, surgeons used a blue dye and a radioactive tracer. They’d inject it near the tumor, then use a handheld gamma probe to hear a clicking sound when they got close. It worked… but it was clunky. The blue dye sometimes stained tissues, and the radioactive stuff required special handling. Plus, you had to rely on sound, not sight. That’s where fluorescence imaging comes in — it lets surgeons see the node glow in real time.
The Magic of Fluorescence: How It Works
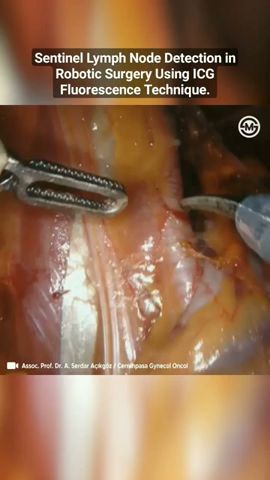
So, how does this wizardry actually work? Well, it’s simpler than you’d think. A fluorescent dye — usually indocyanine green (ICG) — is injected near the tumor. This dye loves to bind to proteins in the lymphatic fluid. Then, a special camera system shines near-infrared light onto the area. The dye absorbs that light and re-emits it at a different wavelength. The camera picks up that glow, and voilà — the sentinel node lights up like a firefly on a summer night.
The cool part? Near-infrared light penetrates deeper than visible light. So even if the node is hiding under a layer of fat or tissue, it still shines through. Surgeons can see it on a monitor, guiding their incisions with precision. It’s like having X-ray vision, but without the radiation.
Why ICG is the Go-To Dye
Indocyanine green isn’t new — it’s been used for decades in liver function tests and retinal angiography. But for lymph node mapping? It’s a star. It’s safe, with a very low allergy risk. It clears from the body quickly via the liver. And it gives a bright, clear signal that lasts long enough for surgery but fades before causing any trouble. Honestly, it’s kind of perfect for the job.
Where It Shines: Real-World Applications
You’re probably wondering — where is this being used right now? Well, it’s already making waves in several cancer surgeries:
- Breast cancer: This is the big one. Fluorescence imaging helps find sentinel nodes in the armpit with high accuracy. Studies show it’s as good as — sometimes better than — the old blue dye method.
- Melanoma: For skin cancers, finding the right node can be tricky because drainage patterns vary. Fluorescence gives real-time visual guidance.
- Gynecologic cancers: In cervical and endometrial cancers, it’s becoming standard for pelvic lymph node mapping.
- Head and neck cancers: These areas are a maze of nerves and vessels. Fluorescence helps avoid collateral damage.
- Gastric and colorectal cancers: It’s emerging as a tool for more precise staging in abdominal surgeries.
Each of these applications has its own quirks. For example, in breast cancer, the dye is injected around the areola. In melanoma, it’s injected near the tumor site. But the principle is the same: light up the node, cut with confidence.
Pros and Cons: A Quick Reality Check
Nothing’s perfect, right? Fluorescence imaging has some serious upsides, but a few downsides too. Let’s break it down.
| Pros | Cons |
|---|---|
| Real-time visual guidance — no guesswork | Requires specialized camera equipment (costly) |
| No radiation exposure for patient or staff | Dye can sometimes cause false positives (e.g., inflamed nodes) |
| Deeper tissue penetration than visible dyes | Learning curve for surgeons new to the tech |
| Faster procedure times in many cases | Not all hospitals have the equipment yet |
| Can be combined with other dyes for dual mapping | ICG is contraindicated in patients with iodine allergies |
That said, the pros usually outweigh the cons — especially in complex cases where every millimeter counts. And as the tech gets cheaper, more hospitals are adopting it.
Comparing Fluorescence to the Old Guard
Let’s be real for a second. The traditional method — blue dye plus radioactive tracer — has been around for decades. It works. But it’s not exactly elegant. The blue dye can stain the skin for weeks, and the radioactive tracer requires a nuclear medicine team to prepare it. Plus, the gamma probe gives you an audio cue, not a visual one. You’re basically playing “hot and cold” with a beeping device.
Fluorescence imaging flips that script. You see the node glowing on a screen. You see the lymphatic channels leading to it. It’s intuitive. It’s like the difference between navigating with a map and navigating with a GPS that shows you the actual road. Sure, both get you there — but one is a whole lot less stressful.
What About Dual Mapping?
Some surgeons use both fluorescence and radioactive tracers together — a “belt and suspenders” approach. It’s not uncommon in breast cancer surgery. The fluorescence gives you the visual, the gamma probe gives you the audio confirmation. It’s overkill for some, but for tricky cases? It’s peace of mind. And honestly, you can’t put a price on that.
Current Trends and Pain Points
Here’s where things get interesting. The biggest pain point right now? Cost. The camera systems — like the Stryker SPY or the Novadaq PINPOINT — can run into the hundreds of thousands of dollars. That’s a tough sell for smaller hospitals. But prices are dropping as competition heats up. And some companies are developing disposable, low-cost fluorescence probes that plug into existing laparoscopes. That could be a game-changer.
Another trend is the move toward multispectral imaging. That means using multiple dyes at once — one for lymph nodes, another for blood vessels or nerves. It’s like having a color-coded map of the surgical field. Imagine seeing the sentinel node in green, the ureters in blue, and the arteries in red. That’s not sci-fi — it’s being tested in clinical trials right now.
And then there’s the push for AI-assisted interpretation. Some systems are starting to use machine learning to automatically highlight suspicious nodes or differentiate between lymphatic tissue and scar tissue. It’s early days, but the potential is huge — especially for less experienced surgeons.
A Thought-Provoking Wrinkle: The “False Positive” Problem
One thing that bugs some surgeons is the issue of false positives. ICG can accumulate in inflamed or reactive lymph nodes — not just cancerous ones. So a glowing node might not always be the sentinel node you’re after. It could be a node that’s just angry from a recent infection or even the injection itself. That’s why fluorescence is best used as a guide, not a definitive diagnosis. You still need to biopsy the node. The glow just tells you where to look.
But here’s the thing — even with that limitation, it’s still better than blindly digging around. And as dyes get more specific (some are being developed to target cancer cells directly), that false positive rate will likely shrink.
What’s Next? The Future Glows Bright
I think we’re just scratching the surface. Researchers are working on targeted fluorescent probes that bind to specific cancer markers — like folate receptors in ovarian cancer or PSMA in prostate cancer. That would let surgeons see not just the node, but whether it’s actually cancerous. Imagine that — real-time pathology without waiting for a frozen section.
Also on the horizon: wearable fluorescence goggles. Yep, you read that right. Instead of a big cart with a monitor, surgeons could wear lightweight goggles that overlay the fluorescent image directly onto their field of view. It’s like augmented reality for the OR. Some prototypes are already being tested.
And let’s not forget cost reduction. As the tech matures, it’ll become more accessible. In five to ten years, fluorescence imaging might be as standard as the scalpel. That’s not wishful thinking — it’s the natural trajectory of surgical innovation.
Wrapping It Up (Without the Fluff)
Intraoperative fluorescence imaging for sentinel lymph node mapping isn’t just a cool gadget — it’s a fundamental shift in how surgeons see the battlefield. It replaces guesswork with clarity, beeps with visuals, and radiation with light. Sure, it has its quirks — cost, learning curves, the occasional false positive — but the trajectory is undeniable.
The real question isn’t whether this tech will become standard. It’s how quickly we can get it into every OR, for every patient who needs it. Because when you’re fighting cancer, every advantage matters. And sometimes, all you need is a little light.